

The Central Nervous System Part 2
Miscommunication

Miscommunication
Have you ever had a major head/neck trauma? Fallen down? Car accident? Got into a fight? Sports injuries? Concussions? Being a kid? Ever been born? Do they not YANK on the head and neck to pull you out at birth? With a decent degree of force (but sometimes all it takes is a force in a certain direction) and now all of a sudden your upper cervical vertebrae are not articulating correctly, they shift out of place, and encroach on that space where the blood vessels, CSF, and brainstem/spinal cord exist.
If you’re only misaligned a little (1mm or so) the first thing you’re going to compress is the CSF and blood vessels creating a narrower channel for the fluid to flow.
If you kink off a hose, even a little, do you not alter the rate, direction, and pressure of the flow?
>No. Pascal’s Law states that a force applied to a fluid will transfer in all directions equally. Think of the ripple in a pond after throwing a stone in it.
If you have a disruption or any kind of blockage of CSF flow into the brain and down the spinal cord, or a change in the rate, direction, or volume of the flow, will you:
Create a build-up of intracranial pressure from the CSF inside the brain?
>Yes. Behind the eyes this is glaucoma. Behind the cerebellum it can result in Chiari Malformation.
Be able to fully and properly turnover the CSF to maintain its functions?
>No.
Be able to fully and properly transport neuroendocrine hormones from the pituitary gland and the pineal gland to their target organs?
>No.
Have a problem with ANY (and or ALL) of the neuroendocrine hormone pathways? (go back to Part 1 and look how many there are and what they do)
>Yes.
Be able to fully and properly transport neurotransmitters in the CNS like dopamine (movement, memory and pleasurable reward and motivation), serotonin (mood, sleep, digestion, nausea, wound healing, bone health, blood clotting, and sexual desire), GABA (reduce neuronal excitability by inhibiting nerve transmission), glutamate (learning and memory) and all other neurotransmitters?
> No.
Have potential for impaired cognitive function? Depression? Anxiety? Poor health and wound healing of all tissues including the brain? Decreased motivation? Decreased memory? Decreased restful and fruitful sleep? Decreased sexual desire? Mind racing; unable to shut it off? Stress? How many more can we list here? Don’t think I can fit an encyclopedia’s worth of information on this one article.
>Yes.
Be able to fully and properly transport the special “building blocks”, nutrients, and healing properties to damaged areas of the CNS?
>No.
Be able to fully and properly clean out the metabolic waste and heavy metals?
>No.
Be able to fully and properly heal and repair the brain from brain damage or dysfunction?
>No.
Be able to heal and repair from neurodegenerative dis-ease processes?
>No.
At what percentage loss of rate/direction/volume of CSF flow do problems occur?
>Any? The state of the dis-eased condition is directly related to the degree and duration of its percentage loss.
>A large percentage + any time = A BIG PROBLEM.
>A small percentage + a long time = An ever-progressing problem.
If you compress into the space of the CSF further with a bigger misalignment you can lead to compression of the transition of the brainstem and upper spinal cord. Fluids can’t be compressed (think hydraulics) but if a force is applied externally the force will transfer in all directions away from the compressive force (Pascal’s Law)—in this case the transition between the brainstem and the upper spinal cord…. that carries virtually every nerve from your entire body and also houses the major cranial nerves…. as well as change the direction and the rate/volume of the flow of CSF. Compounding problems.
If you compress a nerve, the nerve can no longer send a signal properly, either sensory input and/or motor output, and it will result in pain and “symptoms” of dysfunction. This means everything that nerve attaches to, detects and sends information from, controls the function of, and otherwise regulates, regenerates, immunomodulates, and controls the homeostatic state of will also have a problem.
So any one of these major cranial nerves can be affected?
Go back and read (how many things do those cranial nerves do?).
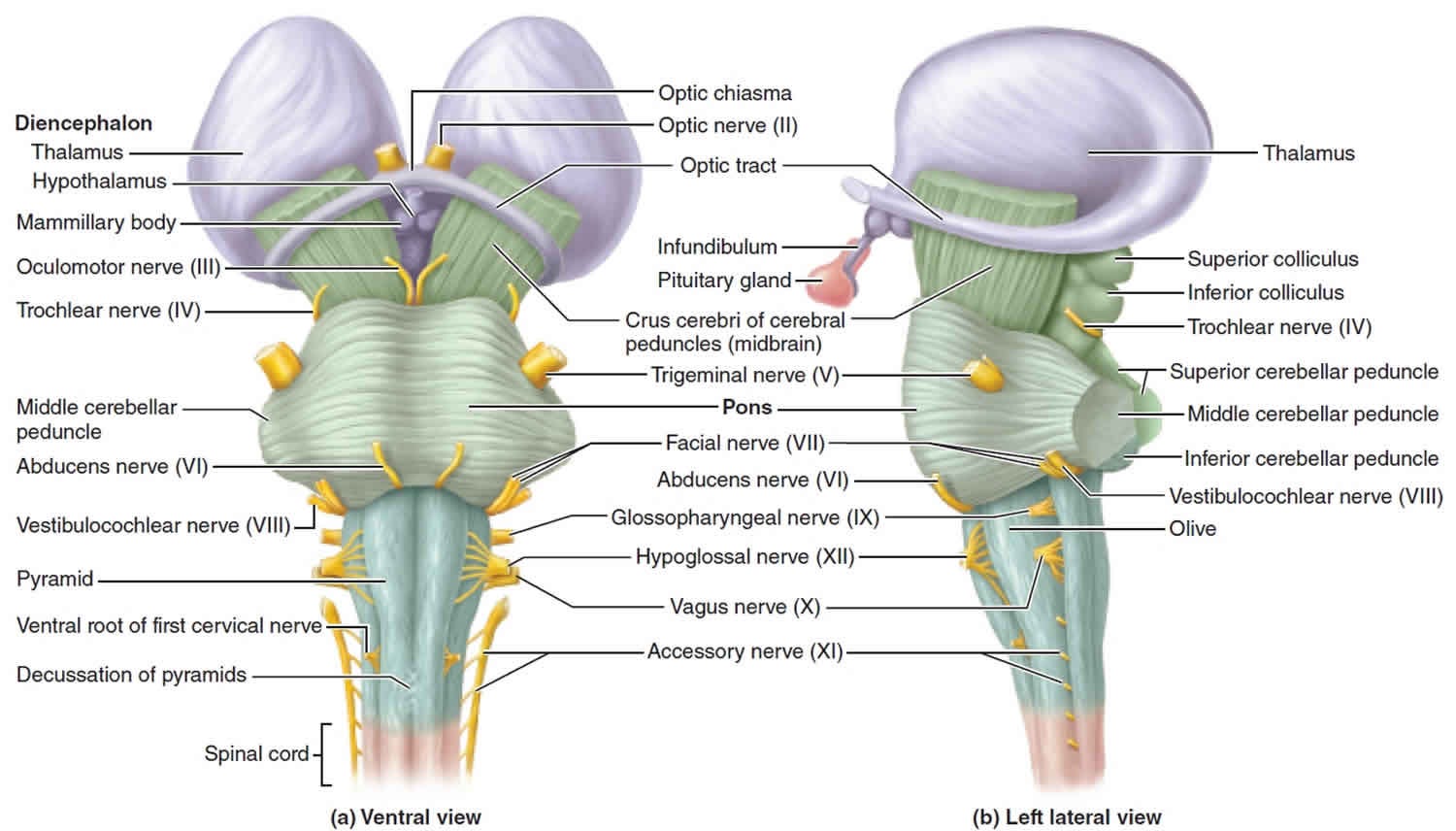
What about the tissues these nerves travel to?
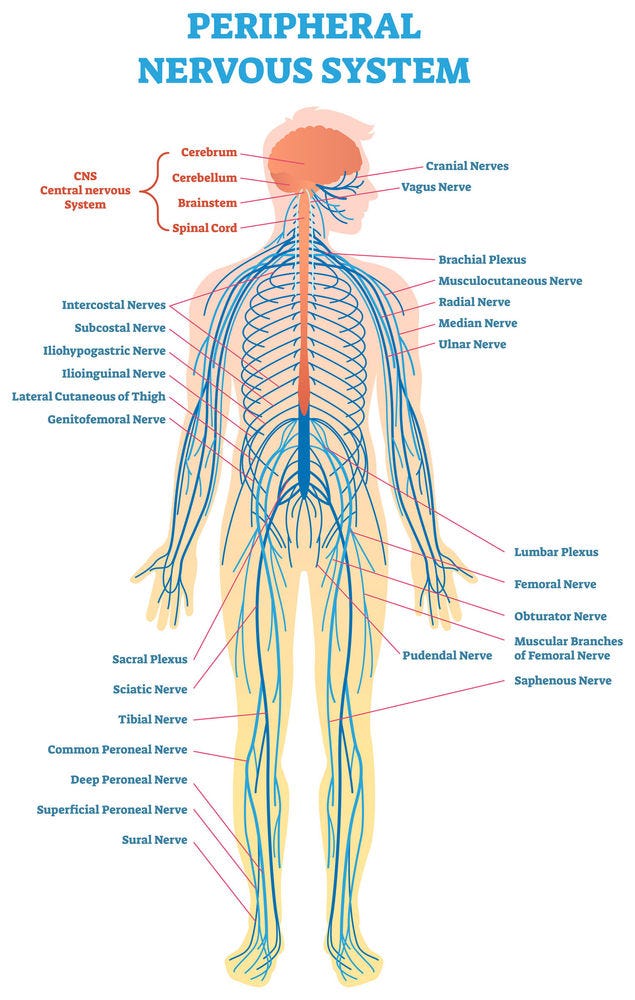
Compression of these nerves results in all of the aforementioned nerve compression symptoms/dysfunctions but can also lead to intense pain, numbness and tingling, as well as loss of strength and function of the tissues these nerves go to.
And lastly, how many major parasympathetic nerves exist in the upper cervical/brainstem?
Virtually all of them?
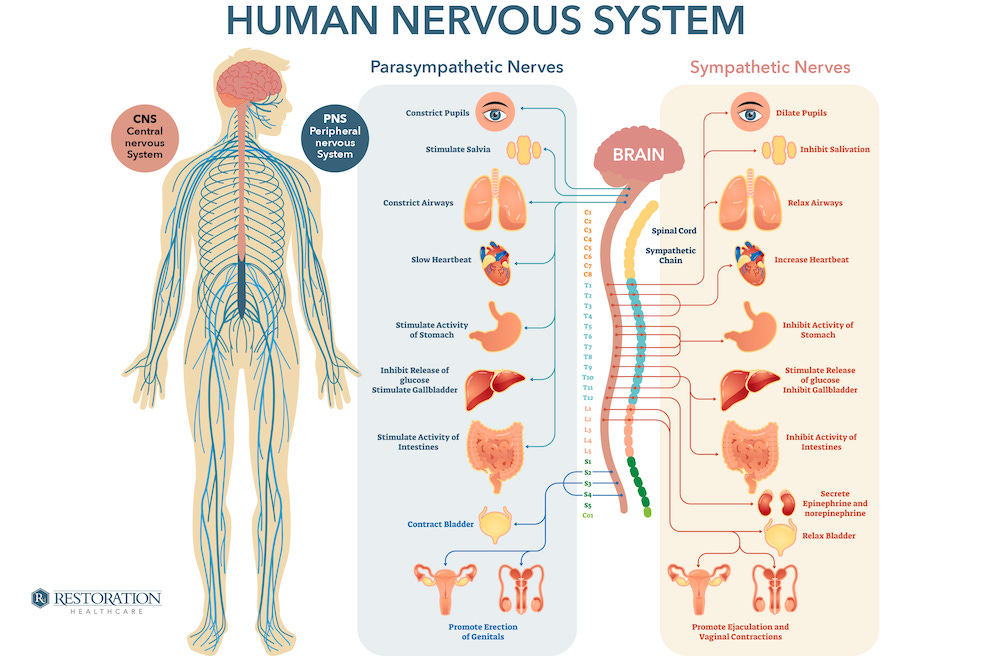
If you are compressing on parasympathetic nerves can they function properly?
>No.
Will you have a problem getting back into parasympathetic/rest-and-digest/homeostasis/anabolic state?
>Yes.
If you are stuck in Sympathetic overdrive, can’t get into PS/homeostasis/anabolism will you constantly be operating in a state of “fight or flight”?
>Yes.
What’s that otherwise known as?
>Dis-ease. Or disease.
How many dis-eases can be caused or perpetuated JUST by CSF/Upper Cervical/Brainstem compression due to misalignment? All of them?
>Think about that for a second. (and we’re not even done)
This compression isn’t some pinched nerve in your low back causing sciatica, this is your brainstem and confluence of all nerves - it’s a BIG PROBLEM that threatens your body’s survival. But when survival is at stake (your body’s number one goal is to survive) your body is willing to make sacrifices to keep you alive.
As an example everyone is familiar with—let’s take temperature regulation. If you go outside in the cold weather and stay put your body will fight the change in external temperature in order to maintain its internal temperature. (Where does temperature regulation occur? In the hypothalamus just north of the brainstem.) You will start going through catabolism (burning fuel), your muscles will shiver in order to create heat as a byproduct, and your foreman will tell the blood vessels in your extremities to shunt blood back to the internal organs and the central nervous system. So what are the first things to get frostbite? Fingers, toes, ears, and nose—those with the least amount of blood supply, and those with the least amount of necessity for your survival.
This was a sacrifice the body made in order to survive. Your internal organs and nervous system are WAY more important than your ears and toes etc. You can live without fingers and toes but you can NOT live without your internal organs or nervous system. Therefore the body KNOWS there is a system of hierarchy of your tissues/organ importance and already ranks their values to your survival.
So, what’s more important than your Brain, brainstem, and CSF? What’s higher on the hierarchy?
>Nothing.
So, what’s the CNS willing to sacrifice to keep its function and survival?
>Anything.
And it does. It does indeed make a sacrifice.
Let’s take a look.
Do you think this person has an upper cervical misalignment? (Yes, they do.)
The problem of brainstem/CSF compression can be managed by altering the path of the neural tube—you get a kink and on one side you will see a lift. The brain will then direct the paraspinal muscles to pull the spine away in order to open up the neural tube and relieve compression. It will also direct the upper trapezius muscle, suboccipital triangle muscles, and the SCMs to contract to keep the eyes on the horizon (can’t traverse the world tilted). Think of it like a cell tower—they have cables tying it down to the ground in many directions. If they are all of the same tension then the tower stands straight up. But if you cut a few of the cables then the tower will lean to the side that has more tension on it now. The same (sort of) thing happens in the paraspinal muscles. The brain increases the tension on one side of the paraspinals and decreases it on the other, and the result is the spine shifts over to that side (remember this for later).
If the spine moves over to one side (you can’t traverse the world tilted very well) it’s going to have to compensate by also going the other direction to balance it out.
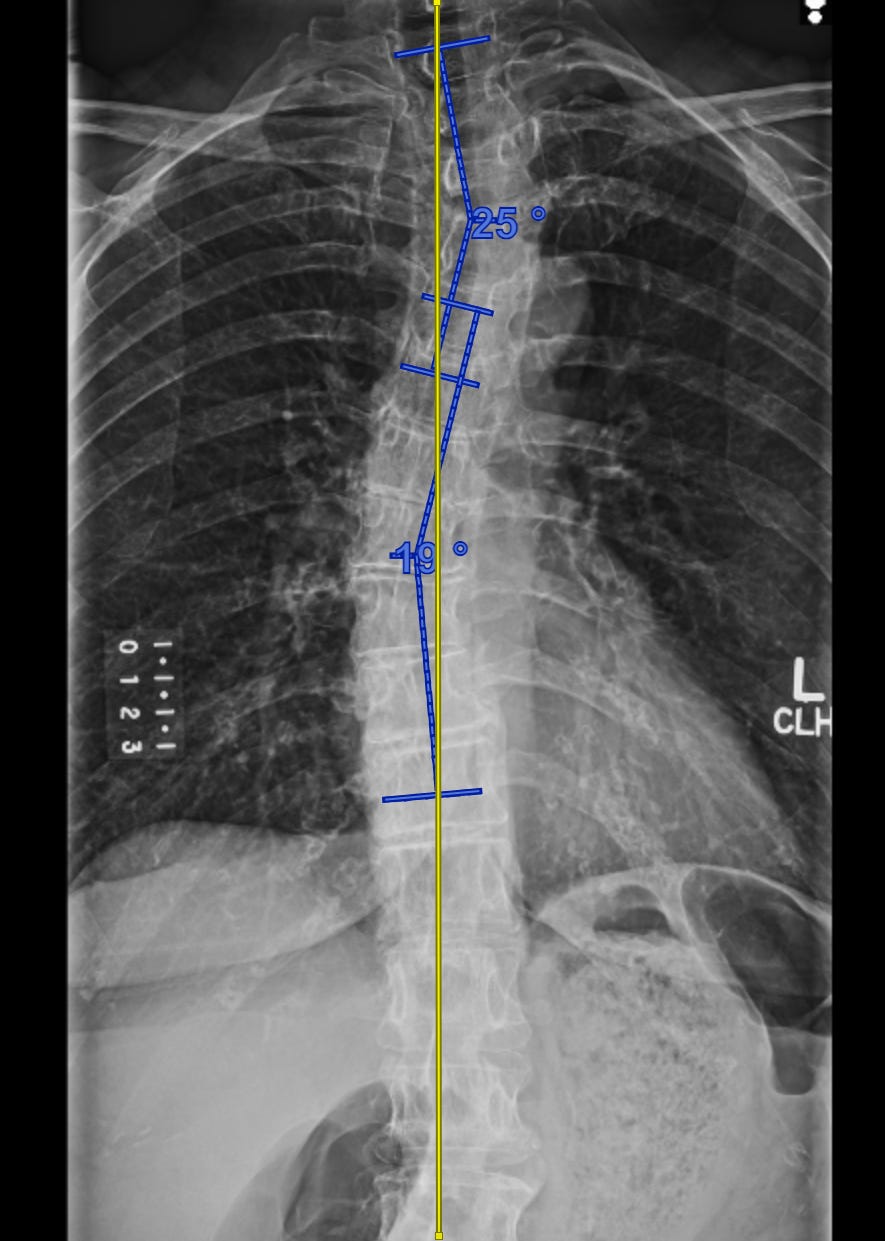
And so it does. Back the other direction
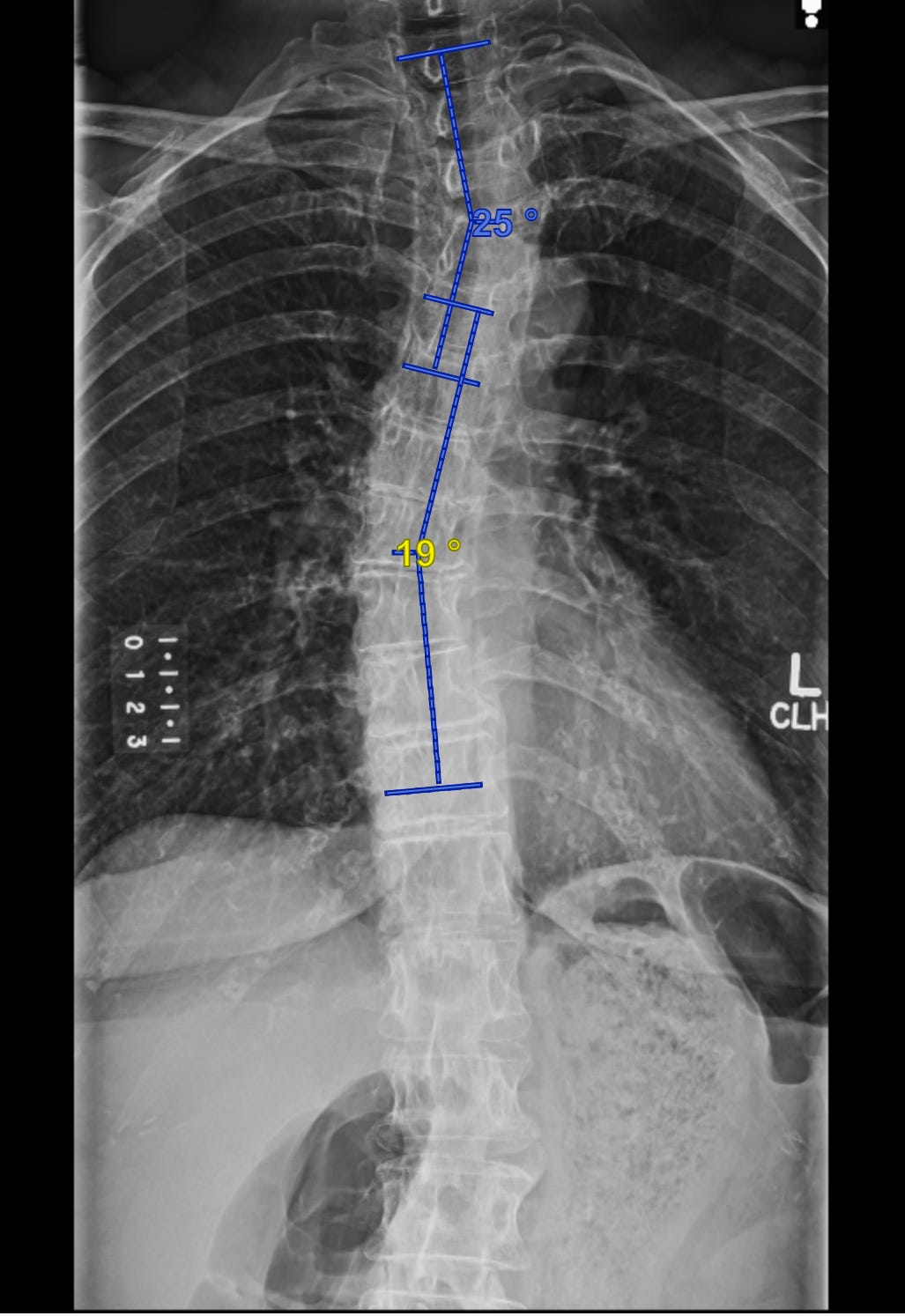
And back again.
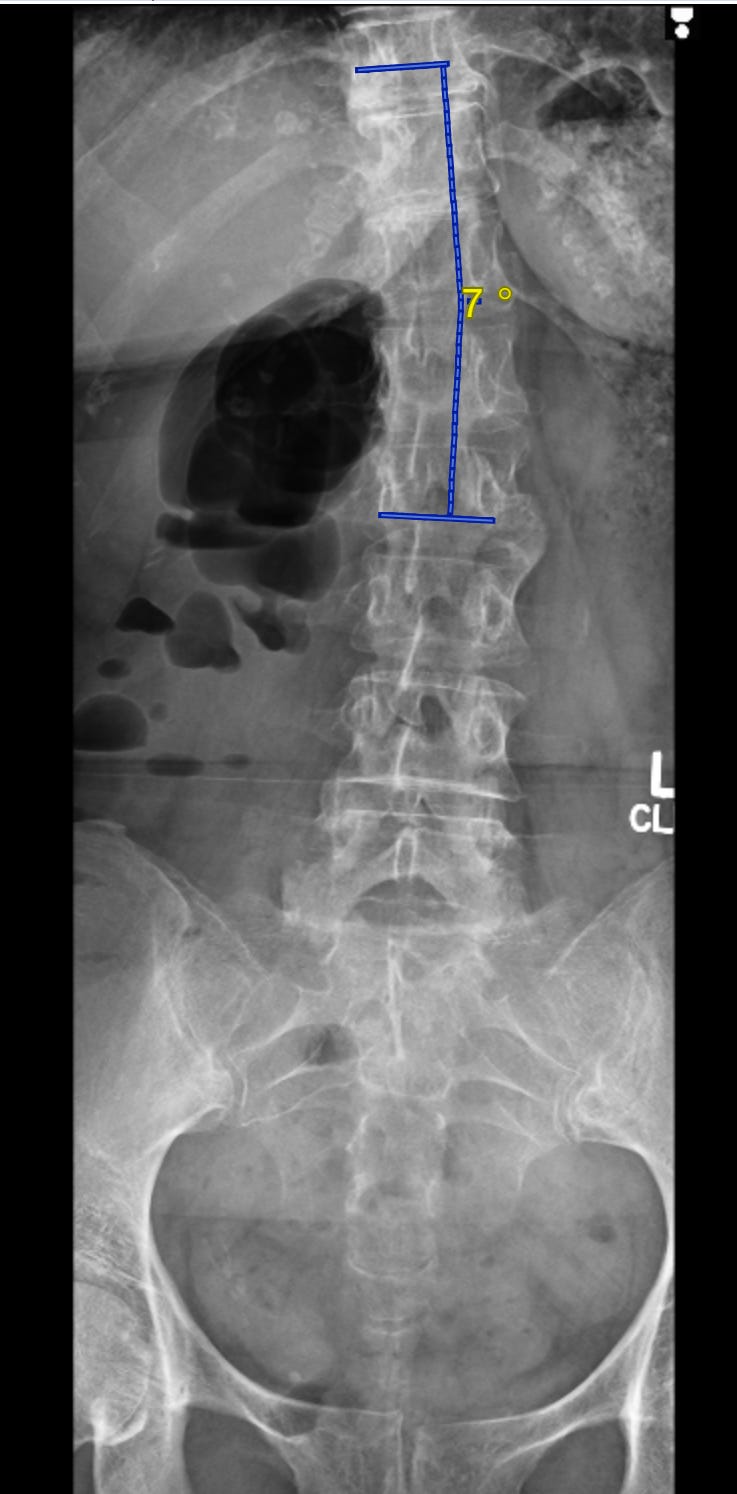
These images are all the same person and a real patient at my office. Do you think she has dis-ease? Pain? Where? A lot of places?
This is called a “compensatory scoliosis”. Compensatory because it is compensating for upper cervical misalignment and the resulting kinking off of the neural tube and its contents. The vast and overwhelming majority of people who have scoliosis have a compensatory scoliosis. If you have upper cervical misalignment- you have a compensatory scoliosis. The congenital form is due to malformed vertebrae causing uneven stacking of the next vertebrae above or below, but this is considered “rare”.
How does it get there? The CNS tells the paraspinal muscles to asymmetrically contract in order to bring the spine into a very specific position that directly matches the upper cervical (UC) misalignment. By moving the vertebra below you can open up the neural tube to mitigate the kinked brainstem above due to UC misalignment.
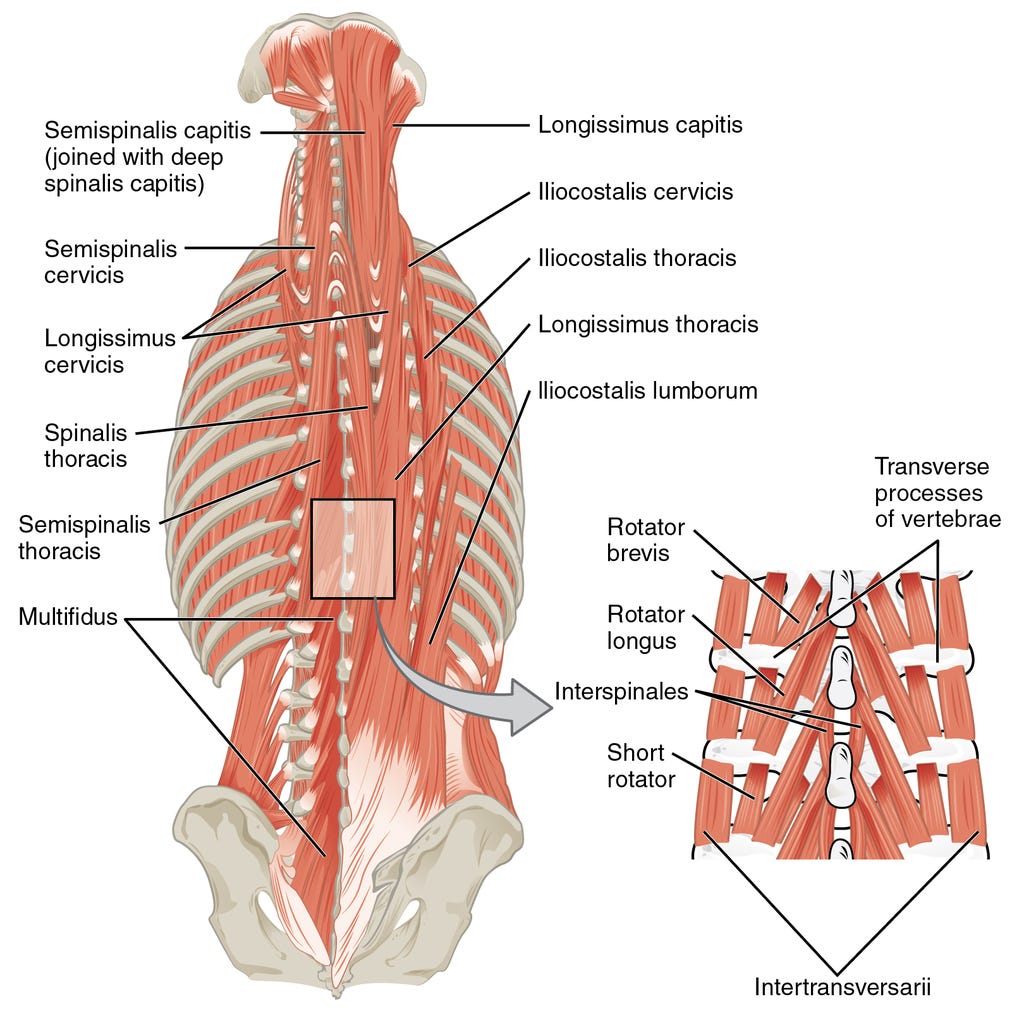
These muscles traverse both sides of the spine, some big and some small, and when they asymmetrically contract they can create the specific and necessary tension to manifest the compensatory scoliosis. Everyone who has an upper cervical misalignment has a compensatory scoliosis. The degree of which is directly associated with the degree of UC misalignment.
Once misaligned in the upper cervical spine, and after the spine below compensates by forming a scoliosis to match it, you can have another trauma on a later date in a different direction that misaligns you FROM a misaligned position. Your spine below will also have to compensate FROM a compensated position. This “stacks on top” of the misalignment below without removing it— this is what we refer to as a “layer”.
Each layer has its own torque on the spine that brings it out of neutral.
These sacrifices, of course, have its own set of consequences because while the spine changed shapes and positions the force of gravity did NOT.
The spine is designed to be vertically straight (with built in normal front to back curves to increase strength) so that you CAN handle the ninety-degree, direct, compressive force of gravity on the body. Its vertebrae are designed to be cube shaped to handle it and disperse the force over a larger surface. Furthermore, there are ‘discs’ in between each vertebrae to act as shock absorbers. The disc contains a “jelly fluid” encased in many layers of connective tissue (annular fibers) wrapped around it similar to a Chinese finger-trap design (can’t compress a fluid; hydraulics).
But now the spine is not able to handle those vertical compression forces very well because their position has changed. On one side of the spine the connective joints and vertebrae are pulled apart and on the other side they’re compressed—experiencing asymmetrical dispersion of forces.
And if you squeeze a balloon on one side, what do you think happens?
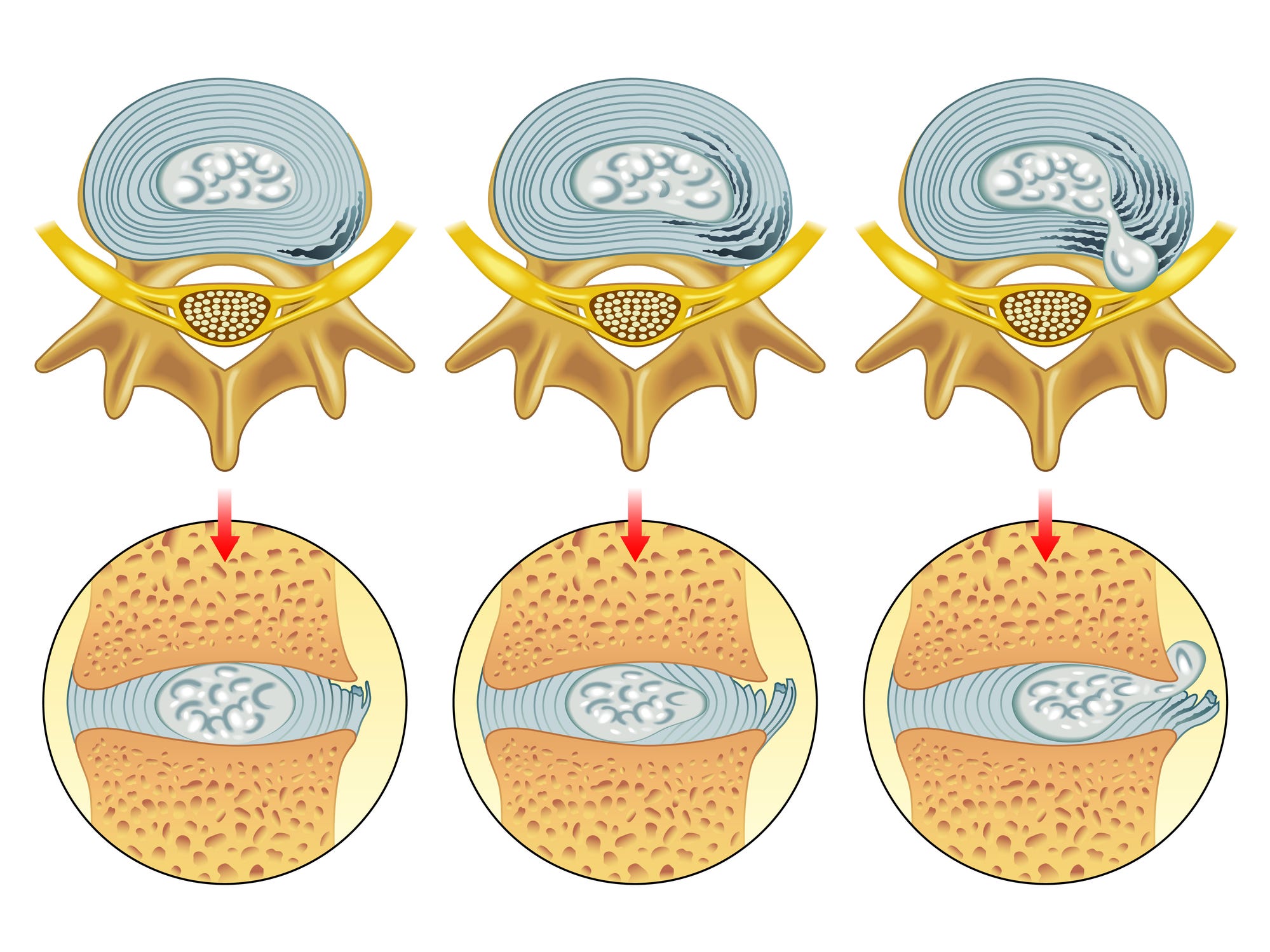
On the gapped side the joint capsules and ligaments become stretched, and the ‘disc’ “balloons” out.
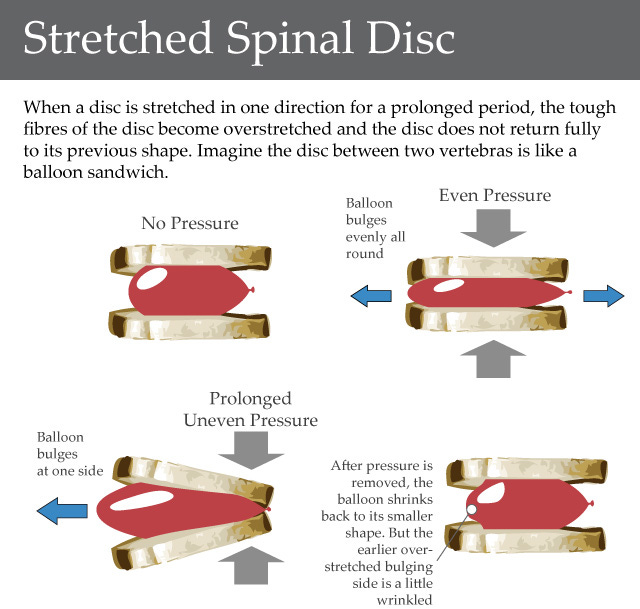
If this force continues, or is great enough, the fluid (that can’t be compressed) will push through and tear the annular fibers. If it reaches the outer edge it will cause a “herniation”. Due to the proximity of the spinal cord and spinal nerves exiting bilaterally at all vertebral levels of the spine this can cause a series of consequences of its own.
The greater the asymmetrical and compression force experienced, along with the duration and constant state of which the spine experiences these forces causes progressive destruction of tissues and “dis-ease”.
This is diagram is showing you some of the stages of “Degenerative Disc Disease”.
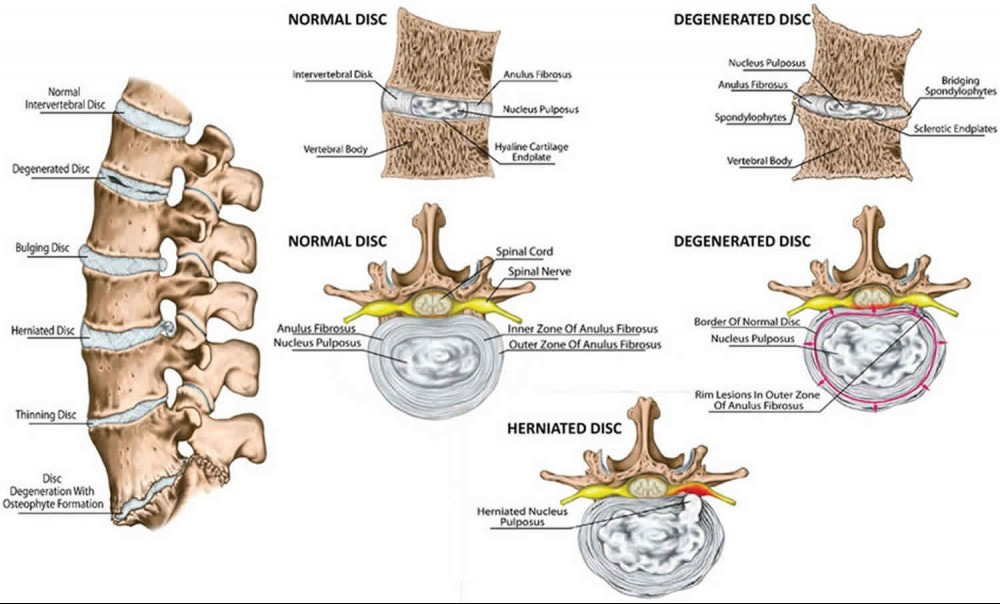
Depending on the degree of bulge/herniation of the disc it can cause the compression of the spinal cord or the nerve traveling out that side it and can lead to first pain, then numbness and tingling, then loss of motor function down the path of that entire nerve and all the tissues it goes to.
In worse cases, the nerve can be compressed coming out of the spine by the disc, and AGAIN as it enters through the foramen magnum—double compressed. Imagine how much function and homeostasis those tissues have from multiple compressions along the path of any nerve.
On the opposite side the opposite is true. Instead of the disc bulging out and the capsules/ligaments stretching, the joints on the other side are being overly compressed. Have you ever used your hands for work? Worked out by lifting weights? What do your hands develop? Callouses. A callous is the body’s response to these forces by growing more tissue in direct response to the stress/force placed on it in order to handle that stress/force better next time.
So if two bones are both experiencing stress/force at a joint what will the result be? Growth of more bone in response? A bone callous?
On x-ray, the more dense an area is the more white it appears, and the less dense an area is the more black it appears. Now find the joints (where one bone meets another) and look at all the extra white? This is increased bone density or “extra bone growth”; a bone callous.

The foreman perceives this scoliotic scenario as spinal instability and so to offer any kind of help at all it’s going to instruct the spine to start fusing together to create stability. The ligaments that attach each vertebrae start to ossify (turn to bone) and the ends of the vertebrae growing out due to the excess compressive force eventually meet up (stalactite and stalagmite) until they join together. These are otherwise known as osteophytes and bone spurs. And what do certain doctors say about bone spurs? Good thing or a bad thing? They say “bad thing—let’s remove them” ….but this was what your body was doing to stabilize its unstable spine holding its very delicate spinal cord (information/control highways).
Did they fix anything by removing them? No.
And if you thought we were done, we aren’t. This scenario hasn’t even taken movement into consideration yet.
Muscles move the body by contracting ONLY—they’re kind of like rubber bands—they contract. Muscles do not actively stretch; muscles are either actively contracted (shortened) or they’re inhibited (lengthened)—and since muscles are always on opposing ends of a joint they create opposing actions and this is how controlled movement occurs. Controlled by what? The foreman.
In order to control movement of a joint there has to be activation of muscle tissue on one side and an inhibition on the other. Therefore, this process is BUILT IN to your system— as soon as one muscle contracts there is a spinal reflex (non-voluntary) that inhibits the opposing muscle—this is automatic.
Knowing that information, when you have an upper cervical misalignment causing compression on your neural tube and its contents your body will contract muscles to move the spine over to “unkink” the flow AND will contract the muscles that attach to it to reduce the range of motion and adjust position while holding the head steady on the horizon to prevent it from getting worse. This means your upper trapezius muscles, SCMs, scalene muscles, and paraspinal muscles will contract and STAY contracted until the problem is resolved.
(How many people are constantly complaining about how “tight” and “tense” their upper shoulders and neck muscles are? How many times have you gotten a massage to try and loosen them up only for them to come back after a period of time? Has it ever worked long-term or fully resolved? Ever?)
If a muscle contracts what MUST happen according to your built in spinal reflex? The opposing muscle must inhibit (turn off). Let’s look at how this plays out in the human body:
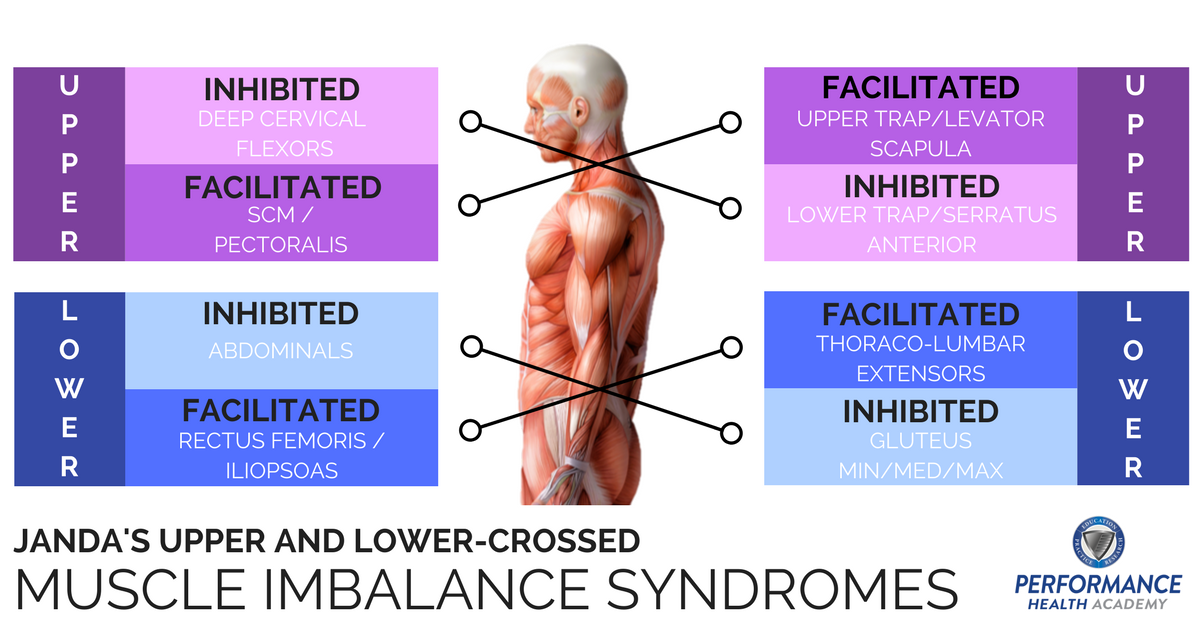
The upper traps/levator scapula contract long term causing an inhibition of their opposing muscles the lower traps/rhomboids/serratus. These inhibited muscles’ jobs are to bring the scapula (shoulder blade) backward and down toward the midline creating stability of the thoracic spine and rib joints, while also stabilizing the shoulder joint. If the shoulders are not positioned down and backward then they are up and forward which means the next set of contracted muscles are the pectoralis muscles. If your shoulders are now up and forward where does your head go? Forward. So the SCM’s also contract to draw the head forward thus inhibiting the deep cervical flexors which are responsible for keeping the ears over the shoulders and holding the cervical spine in line with the rest of the spine. This system perpetuates itself, progressing worse and worse, causing more compressive forces on the spine resulting in more disc and joint degeneration issues.
The same thing can happen in the lower body. The upper cervical misalignment causes torquing of the whole spine leading to low back injury. The last thing that feels good is to extend and stand up straight on a low back injury and thus you sit down or bend at the hips to take the pressure off. The hip flexors contract leading to inhibition of their opposing muscles the glutes which stabilize your center of gravity and pelvis, and hold you erect, forcing you to stand up with your low back muscles (not designed to do this long term). The contraction of your low back erector muscles causes the inhibition of your core musculature which acts to stabilize your lumbar spine like a “corset”—core vs corset…. (the naming of these things, I swear).
If you will notice in the diagram above, all of the “inhibited muscles” are your “postural muscles”. They stabilize your midline and keep you standing erect so that you are able to handle the force of gravity as well as provide a stable foundation for which your limbs/extremities can pivot off of. If the muscles that move your limbs are now also being used to also stabilize the joints (double duty), all while pivoting off of an unstable midline, THEY will go through overuse injuries at the joint, muscles, or tendons. Rotator cuff, biceps tendon, labrum, SI joints, hip joints, hip labrum, impingements, patellar tendinitis, knee injuries, meniscus tears, ligament tears, tendon tears, muscle tears, …and on and on and on…
All of that - again - are just symptoms of a domino effect caused by an upper cervical misalignment. AND if that area’s nerves are also compressed at the upper cervical or at the spine, or anywhere they travel through overused and spastic muscles to get where they need to go, then the level of homeostasis, anabolism, and regeneration that occurs there is precipitously less in a direct ratio compared to the use + loss of communication with the foreman.
Weak muscles? Inability to properly move? Immobility? Lack of range of motion?Poor posture? Overuse injuries? Degeneration? Getting older? Yes, but those are SYMPTOMS— NOT the cause. The cause was the upper cervical misalignment.
You can have problems ANYWHERE along the construction site contributing to the level of degeneration, dysfunction, dis-ease, etc. Workers, supplies/materials, parts and tools, dirty site, poor management, lack of security, and vandalizers, but no matter what you do to address those issues, if you never address the communication issue then the best you can ever do is some percentage less than 100% in direct relation to the duration and level of miscommunication you have. If you go to a “specialist” who doesn’t work “in the whole body” and only address or attempt to correct one of these pieces of the construction site, does anything ever heal? No.
However, if you simply (properly) “unkink” the upper cervical spine and restore the integrity of the neural tube, thus freeing up the CSF/brainstem/spinal cord, what do you think will happen next?
The Upper Cervical Specific Stress Analysis allows for the body to re-establish communication, control, function, and the innate healing/regenerative properties: The whole domino-effect will undo and unravel itself in reverse order, and the dis-eased, degenerative, dysfunctional, etc tissues in the body that were a problem before will begin to heal, regenerate, resolve, and function properly, as written by your DNA.
THIS is called your “innate intelligence” and it exists for everything in your avatar from head to toe.
Perfect in design.
Sweet. How do you do that?
See Part 3:
Note to reader: the information about the chiropractic technique described in these articles is called Upper Cervical Specific and was developed by BJ Palmer. It is implemented through Stress Analysis, which was developed by Guillermo D. Vazquez, D.C. Articles are written with permission of Dr. Vazquez. Opinions outside of the subject matter are my own.
Beautifully presented! I have had great results for myself and children with cervical chiro👏🏼
Beautifully written. Resonates with my soul. Maybe this epiphany was a gift from God for your fantastic work on Humanity's True Biblical History. I was glued to your Telegram posts on that! Look forward to number 3.....The Great (Master) Reset! Thank You for your work to help heal Humanity!